

Long Covid Weekly #50: 50th Edition!, Possible new biomarker? & More
Long Covid Weekly #50: 50th Edition!, Possible new biomarker? & More

Hi everyone,
As you may have seen from the subject line, this is the 50th edition of the Long Covid Weekly! Our journey has been enriched by your continuous support and unwavering belief in the values we champion. To our valued contributors, your vibrant narratives, profound wisdom, and varied perspectives have been the heart of our content, enabling us to provide our readers with a diverse and in-depth understanding of the Long Covid. Here is to 50 more editions of this newsletter, with hopefully a lot more promising research on the way!
In this edition, we explore the diverse manifestations of Long COVID, as a recent study highlights its heterogeneity. Additionally, we showcase the groundbreaking achievements of the UChicago team in winning the NIH Long COVID Computational Challenge. Moreover, we delve into the interplay between blood type and susceptibility to COVID-19 and shed light on the existential and identity challenges faced by individuals living with chronic conditions of Long COVID. This newsletter is packed with valuable information aimed at fostering understanding, support, and improved management of Long COVID.
Media
Article: Long COVID is not a single condition, study finds | Newsroom
SUMMARY:
Long COVID is not a single condition, and should not be treated as such, according to new data collected in a nationwide study released May 31st in the Open Forum of Infectious Diseases.
The study looked at persistent symptoms experienced by patients with COVID-19 both at three- and six-month intervals.
In all, 5,963 patients participated in the study, with 4,504 of the participants testing positive for COVID-19 and 1,459 testing negative.
The four major symptom categories for people who tested positive for COVID-19 included: Minimal symptoms (72% of the cases), Tiredness, headache and muscle/joint aches (17% of cases), Tiredness, headache and muscle/joint aches with loss of taste and smell (5% of cases), Symptoms across multiple systems (6% of cases).
Overall, the study will help determine funding and policy support for long COVID programs.
My Take:
It is important to recognize that long COVID is not a singular condition, but rather a collection of symptoms that can vary over time.
It is kind of crazy that this is only becoming common knowledge now
Article: Long COVID: answers emerge on how many people get better
SUMMARY:
More than three years after SARS-CoV-2 began its global spread, an estimated 65 million or more people are still living with the often devastating effects of long COVID — and scientists are still struggling to understand this complex condition..
The answer to how many people with Long COVID get better depends on various factors, including the definition of Long COVID and the timescale for possible improvement.
One study found that after two years, 17.2% of adults who caught SARS-CoV-2 still had symptoms of Long COVID.
Risk factors for developing Long COVID include being female, older age, high body mass index, smoking, and certain pre-existing diseases such as asthma and diabetes.
The severity of the initial infection may also be a factor.
There is ongoing research into medications that may help prevent or treat Long COVID, such as metformin and the antiviral Paxlovid.
However, more studies are needed to confirm their effectiveness.
Article: UChicago Team Wins NIH Long COVID Computational Challenge
DEFINITIONS:
Rapid Acceleration of Diagnostics (RADx): a program at the National Institutes of Health (NIH) that aims to speed up the development, validation, and commercialization of innovative diagnostics to combat COVID-19.
SUMMARY:
One of the most pressing unanswered questions right now is how to predict which patients will experience Long COVID.
The Rapid Acceleration of Diagnostics Radical program at the National Institutes of Health (NIH) launched the Long COVID Computational Challenge in August of 2022.
Convalesco, a team of scientists from the University of Chicago, won the challenge by developing a lightweight monitoring system using machine learning models that updates a patient’s likelihood for developing Long COVID in real time as new symptoms are reported.
By using machine learning models and real-time symptom monitoring, the team created a visualization dashboard that can help doctors determine the likelihood of a patient developing Long COVID.
The visualization dashboard utilized 100 symptoms and 31 demographic features to build a timeline of the cumulative risk for developing Long COVID.
My Take:
This development by the University of Chicago team is significant as it addresses the challenge of predicting which patients will develop Long COVID
Their success in the Long COVID Computational Challenge shows the potential of AI and machine learning in improving our understanding of COVID-19 and its long-term effects.
The release of their full code as open source allows for further collaboration and advancements in this area.

Article: How Blood Type Can Increase Your Risk of COVID-19 - CNET
DEFINITIONS:
ACE2: A protein found on the surface of cells that the SARS-CoV-2 virus uses to enter and infect the cell.
SUMMARY:
Recent research shows that one particular blood type heightens the risk of infection.
When the SARS-CoV-2 virus, which causes COVID-19, first appeared in 2019, doctors and scientists began to notice a curious association between blood type and infection risk.
Numerous studies investigated the link, dating back to the earliest days of the pandemic.
A new study, published in the journal Blood on June 27, describes a potential mechanism, providing evidence that SARS-CoV-2 preferentially binds to the surface proteins associated with blood group A.
To infect a cell, SARS-CoV-2 uses its spike protein to bind to a protein on the surface of a cell, known as ACE2.
My Take:
It suggests that individuals with blood type A may be more susceptible to infection, while those with blood type O may have some level of protection.
Research
DEFINITIONS:
Existential loss: refers to the disruption of a coherent and stable sense of being-in-the-world due to chronic illness.
Self-narratives: the stories individuals construct about themselves and their lives.
SUMMARY:
Living with chronic or persistent health conditions can disrupt people's identity and raise existential questions about their existence.
Medical sociologists have studied the existential experiences of chronic illness within the parameters of body, biography, time, and uncertainties.
The sociological literature on chronic illness lacks explicit theoretical explanations for the experiences of existential loss and how it is lived and responded to in everyday life.
DEFINITIONS:
Antibody response: The production of antibodies by the immune system in response to the presence of antigens, such as viruses or bacteria.
Epstein-Barr virus (EBV): A common herpesvirus that is associated with infectious mononucleosis.
HSV-1: Herpes simplex virus type 1, which causes cold sores and can also cause genital herpes.
SUMMARY:
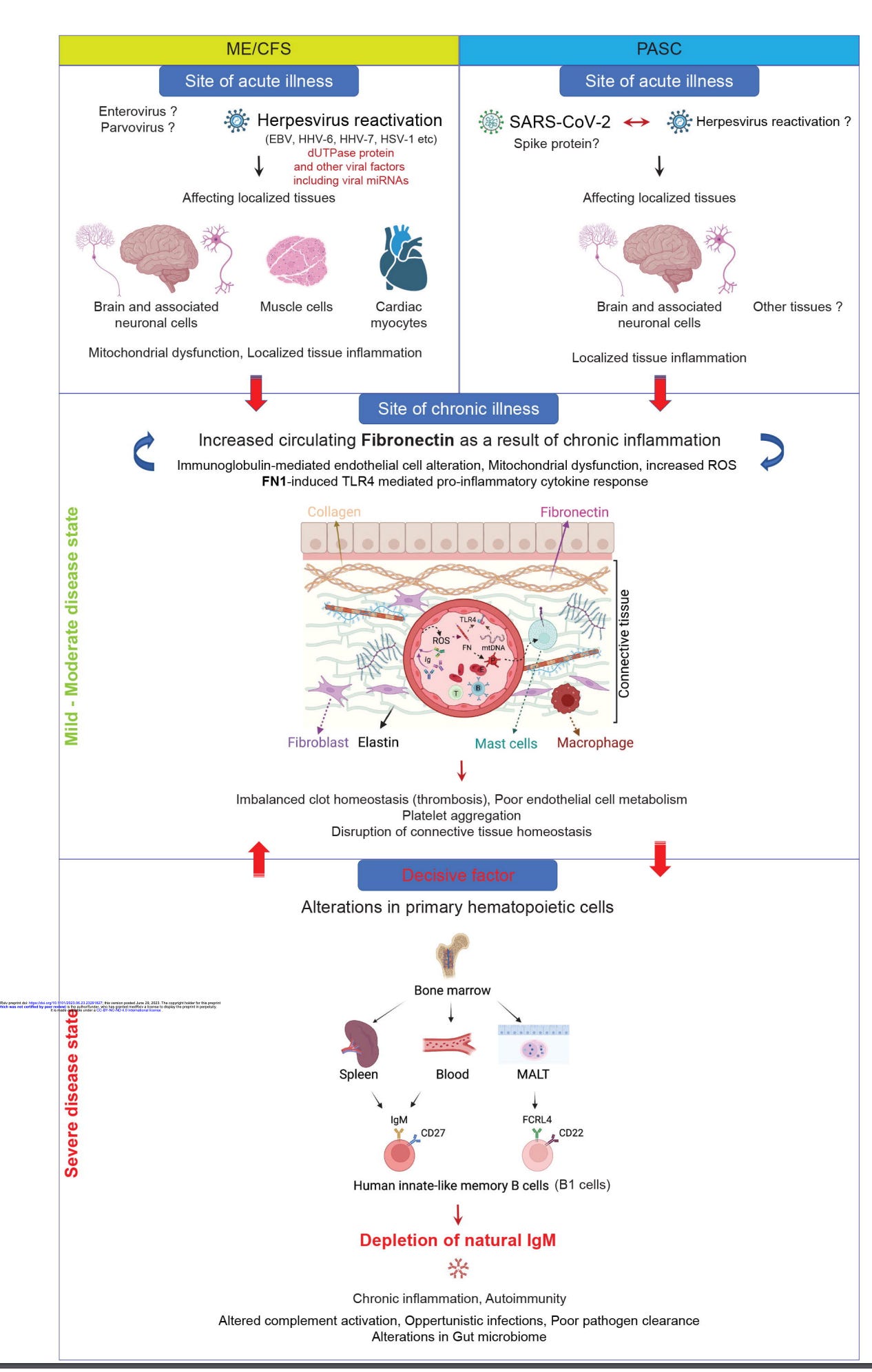
Antibody response to herpesviruses, specifically Epstein-Barr virus (EBV) and HSV-1, is increased in both severe ME/CFS and long COVID patients..
Increased levels of circulating fibronectin (FN1) in serum and depletion of natural IgM against fibronectin ((n)IgM-FN1) are common factors in both ME/CFS and long COVID.
Alterations in host cell cytoskeleton, mitochondrial dysfunction, and oxidative phosphorylation are observed in ME/CFS and Long COVID patients due to herpesvirus dUTPases.
My Take:
The findings of this study suggest that ME/CFS and Long COVID may have similar underlying mechanisms, particularly related to the immune response against herpesviruses and the depletion of natural antibodies.
Further research is needed to validate these findings and explore potential therapeutic approaches targeting herpesvirus dUTPases and the associated alterations in immune response and cellular function.
DEFINITIONS:
Epigenetic: relating to changes in gene expression or cellular phenotype caused by mechanisms other than changes in the underlying DNA sequence.
ACE2: a protein found on the surface of cells in many tissues, including the lungs, heart, and kidneys.It serves as the entry point for the SARS-CoV-2 virus into host cells.
NACE2i: a cell permeable and highly selective ACE2-targeting peptide that inhibits the nuclear translocation of ACE2.
SUMMARY: .
Therapies that complement vaccine-induced immune protection are still needed, especially for vulnerable individuals..
Targeting the nuclear ACE2 pathway significantly inhibits viral replication and prevents early lung inflammation and pathology associated with COVID-19.
NACE2i induces a protective epigenetic ACE2 methylation signature in the bronchiolar epithelium of infected hamsters and in monocytes from blood from vaccinated individuals.
Targeting the nuclear ACE2 pathway represents a means to boost vaccine efficacy and ACE2me might be a useful biomarker to monitor protection.
My Take:
The induction of a protective epigenetic ACE2 methylation signature suggests that targeting the nuclear ACE2 pathway can have long-lasting effects on immune response.
These findings highlight the importance of developing therapeutics that complement vaccines to enhance and prolong protection against COVID-19.

DEFINITIONS:
Postural Orthostatic Tachycardia Syndrome (POTS): an autonomic disorder characterized by a rapid heart rate upon standing without experiencing a significant drop in blood pressure.
Autonomic Dysfunction: impairment or dysregulation of the autonomic nervous system, which controls involuntary bodily functions such as heart rate, breathing, and digestion.
SUMMARY:
Autonomic dysfunction, including postural orthostatic tachycardia syndrome (POTS), is prevalent in patients with Long COVID.
Patients with Long COVID and POTS have reduced respiratory sinus arrhythmia and higher heart rate increase during an active standing test compared to healthy controls.
The COMPASS-31 scores, which measure autonomic symptomology, were significantly higher in patients with Long COVID and POTS compared to healthy controls.
Autonomic testing should be routinely conducted in patients with Long COVID to aid in diagnosis and guide appropriate management to improve health outcomes.
SUMMARY:
The articlediscusses the persistence of SARS-CoV-2 in various populations, including adults, children, and neonates.
It highlights the presence of the virus in children with critical acute illness and raises concerns about the possible biological effects of SARS-CoV-2 or its fragments.
These findings raise the intriguing hypothesis that SARS-CoV-2 fragments can chronically stimulate local immune responses and, through unknown mechanisms, contribute to or be the major pathological event leading to symptoms, including myalgic encephalomyelitis or chronic fatigue syndrome, pains, and other symptoms that characterize Long COVID, or even lead to uncontrolled inflammatory events of multisystem inflammatory syndrome in children
Monocyte CD169: a type I interferon-inducible receptor that is up-regulated during viral infections, including COVID-19.
Neutrophil CD64: an established indicator of sepsis.
Monocyte HLA-DR: an immunologic status marker that decreases during immune exhaustion and is an unfavorable prognostic biomarker in septic patients.
Superimposed bacterial infections can be detected in severe SARS-CoV2-infected patients, indicating the role of bacteria in COVID-19 evolution.
Monocyte CD169, neutrophil CD64, and monocyte HLA-DR expression can be used as predictive biomarkers of SARS-CoV2 outcome in acutely infected patients.
The combined analysis of these indicators can offer a real-time evaluation of patients' immune status and viral disease progression versus superimposed bacterial infections.
This approach can help to better define patients' clinical status and outcomes and guide clinicians' decisions.
My Take:
This study highlights the importance of discriminating between viral and bacterial infections in severe COVID-19 patients.
The expression levels of monocyte CD169, neutrophil CD64, and monocyte HLA-DR can serve as predictive biomarkers for the outcome of SARS-CoV2 infection.
By analyzing these indicators in real-time, clinicians can evaluate patients' immune status, monitor disease progression, and identify the presence of superimposed bacterial infections
Thanks so much for these newsletters! But as someone who just recently recovered from an absolutely devastating six month case of LC ( including POTS/dysautonomia), the amount of research $ on bs topics such as behavioral modification, loss of identity, and observational studies is infuriating. Focus on TREATMENT, cause and prevention. Educate healthcare professionals on identifying/screening patients with long covid POTS using a simple NASA lean test, and educate healthcare professionals about LC, MCAS, fibromyalgia, ME/CFS and PEM. My experience : I was an avid competitive athlete in exceptional good health, fully vaccinated , B+ blood type, slender, no underlying conditions, very mild case of acute Covid. I was an ED RN with 20 years of experience. Looking back, the symptoms of LC with accompanying POTS were glaringly obvious, and this was the beginning of 2023! I had to do months worth of reading of abstracts, and visit numerous Drs and two different clinics to get a diagnosis, a lean test, a cytokine panel, and helpful treatments. I talked my way into getting prescribed paxlovid. Is that what cured me? No one knows because a clinical trial just started in November. But this experience has been humbling and an eye opener in frustration , because I was incredibly, devastatingly sick, and I was pretty much dismissed and treated condescendingly by too many nurses and doctors. I can vividly remember years ago an ER Dr complaining and making fun of a patient with CFS. I had never heard of it before- he stated that CFS is “a diagnosis they give to annoying malingering hypochondriacs that they don’t know what to do with “. Wow. I’m incredibly grateful to those that listened to and helped me, and trying to educate as many people as I can that LC and ME/CFS are real, and what POTS is.
Congratulations! Best such resource on Substack!